In this blog we detailed our just published modelling work on estimating the risk of COVID-19 outbreaks associated with air travel to NZ. We find that the risks are typically very low for travel from Australia (a “green zone” country with small occasional outbreaks from border system failures). But these risks go up if there are larger outbreaks in Australia and especially for travel from other countries (e.g., from an “amber zone” country like Japan or a “red zone” country as per the US during 2020) where rigorous border controls including 14-day quarantine are still required. With the spread of more infectious SARS-CoV-2 variants it is critical that very rigorous ongoing scientific risk assessment is used for NZ and all aspects of border control are optimised for the differing risk posed by green, amber and red zone countries.
We have just published a modelling study in “Scientific Reports”, a peer-reviewed open access journal.1 In this work we aimed to estimate the risk of COVID-19 outbreaks associated with air travel to NZ, along with the impact of various control measures (with and without quarantine). As noted previously,2 risk assessment can be used to stratify the risk of SARS-CoV-2 virus importation and outbreaks in NZ from arriving passengers based on the level of virus transmission and other factors in the source country. This approach allows source countries to be classified using a traffic-lights system into green, amber and red to guide a consistent and proportionate response to border management.
In our new modelling study, we first considered historical data for Australia during 2020 and early 2021 (this being equivalent to an outbreak generating 74 new infections/day) and one flight per day to NZ with no control interventions in place. This source gave a 96% probability of an outbreak in NZ within a year, with a median time to an outbreak of 2.5 months (95% range of simulation results: 3 days to 1.1 years). This risk was equivalent to an average of 110 flights to result in an outbreak. However, the risk could be substantially reduced by a package of non-quarantine measures. That is the combined use of a pre-flight PCR test of saliva, three subsequent PCR tests (on days 1, 3 & 12 while in the community in NZ), and various other interventions (such as mask use and contact tracing), would reduce this risk to 37% probability of an outbreak in NZ within a year (equivalent to a median time to an outbreak of 1.5 years and after an average of 800 flights). Nevertheless, a pre-flight test plus 14 days quarantine was an even more effective strategy (i.e., equivalent results were: 13% probability, 4.9 years, or after 2590 flights).
But more realistically (as more like the situation in mid-2021) we also considered a much lower prevalence of infection with the pandemic virus in Australia – representing only two new infections in the community per week in the whole country. This situation could be generated by ongoing small outbreaks from border system failures. This source, with no border control interventions in place, gave an estimated risk of an outbreak in NZ of only 1.2% per year. This was equivalent to a median time to an outbreak of 56 years (or after an average of 29,400 flights).
In contrast to travel from Australia (a “green zone” country), the risks associated with travellers to NZ from an “amber zone” country like Japan and from the US (a “red zone” country during 2020) were estimated to be very much higher and would definitely need measures such as 14 or 21 day quarantine to substantially reduce the risk. Despite these measures, the high prevalence of infection for the US used in our modelling meant that, even with 14-day quarantine, the risk of an outbreak in one year was 100%, and the median time to an outbreak was only 20 days (or after an average of 29 flights). The equivalent values for Japan were more favourable (34% probability, 1.7 years, or after 870 flights).
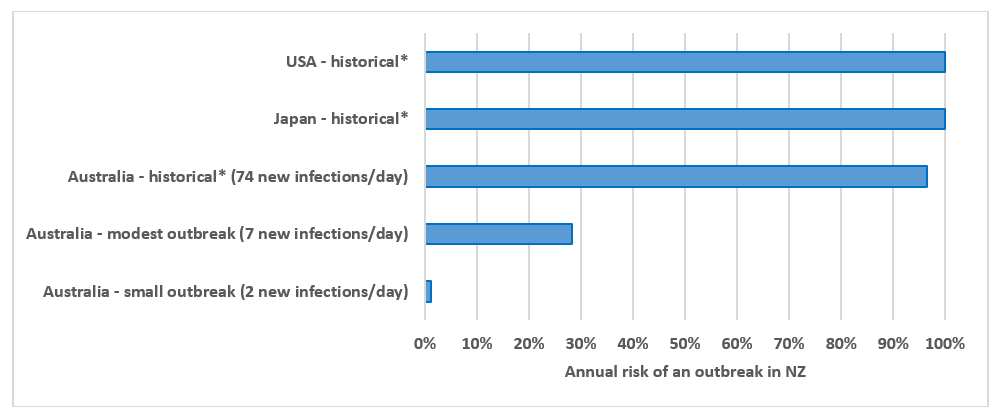
The risk of outbreaks in NZ associated with travel from the various countries can be compared visually in Figures 1 and 2 below. Far more detailed results that also consider the non-quarantine and quarantine based interventions are in our published paper.1
Figure 1: Annual risk of a COVID-19 outbreak in NZ assuming one flight per day from different countries and with no control interventions in place other than mandatory mask use on all flights (and assuming unvaccinated populations)
* Based on historical data on average reported cases of COVID-19 infection over the 1 April 2020 to 25 February 2021 period. See the published paper1 for further details, especially on the impact of both non-quarantine and quarantine-based control measures.
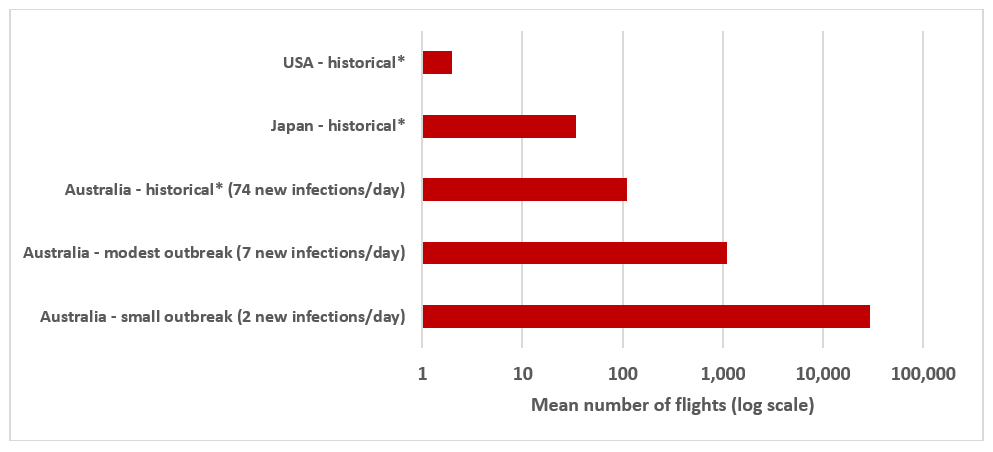
Figure 2: Mean number of incoming flights from different countries estimated to generate a COVID-19 outbreak in NZ when no control interventions were in place other than mandatory mask use on all flights (and assuming unvaccinated populations)
* See footnotes for Figure 1.
Discussion
The risks calculated in this analysis will certainly change over time. They should be reduced if more people in the source countries for travellers and in NZ get vaccinated (although this protection depends on the effectiveness of vaccines against new variants). But before this happens to a substantive degree, the risks might even temporarily increase with the spread of more infectious variants (e.g., the B.1.617.1 currently spreading in Melbourne3) and if international travel volumes are increased.
Nevertheless, our analyses suggest that a quarantine-free travel bubble (green zone) with Australia as per the mid-2021 situation is typically very safe, even with occasional small outbreaks. But where there is large uncertainty about outbreak size in Australia (as per the situation in late May 2021) – it seems very prudent for air travel to NZ to be temporarily suspended from the relevant Australian state or territory as per the recent actions of the NZ Government.
If there were frequent outbreaks in Australia, then NZ could consider adding in some of the non-quarantine interventions we have modelled around pre-flight and post-flight testing and requiring mask use for the first two weeks in NZ. But currently for amber zone countries such as Japan and probably the US at present given its progress with vaccination (although in 2020 we classified the US as a red zone country), we see no viable alternative to 14-day quarantine. Added to this could be tighter constraints on traveller numbers, especially for red zone countries.
As with all modelling studies, this one has various limitations as detailed in our published paper.1 But a key one was that we assumed quarantine only failed due to a tiny proportion of cases having very long incubation periods. In reality, however, NZ has had regular system failures with its border quarantine system with facility workers and travellers in the facilities becoming infected.4 This vulnerability is partly because NZ uses hotels instead of purpose-built facilities and does not confine the travellers to their rooms (i.e., there are shared corridors, lifts, exercise areas and smoking areas). Similar problems occur with the equivalent facilities in Australia5 – except for the more appropriately designed facility at Howard Springs near Darwin. However, these system failures may decline with the increased vaccination coverage of border workers and other ongoing system improvements (see here for a typology of hazards and system failures in the NZ border control system6).
Conclusions
This modelling study suggests that the risk of an outbreak in NZ is extremely dependent on the source country of the incoming travellers. We find that for the current (mid-2021) Australian situation the risk associated with quarantine-free travel from Australia to NZ is very low. But in the situation of Australia experiencing ongoing large outbreaks, the risk could still potentially be reduced to acceptable levels with a package of multi-layered interventions (particularly with repeated testing and mask use) and still with no quarantine. Nevertheless, quarantine is likely to remain important where the source country has high disease burdens (e.g., amber and red zone countries). Also with the spread of more infectious variants, it is critical that ongoing and very rigorous scientific risk assessment is used for NZ decision-making. Also, that all aspects of border control are appropriately optimised for the differing risk posed by green, amber, and red zone countries.
*Author details: Prof Wilson and Prof Baker are at the University of Otago, Wellington. Prof Eichner is with Epimos GmbH, Germany; and with the Institute for Clinical Epidemiology and Applied Biometry, University of Tübingen, Germany.
Image by James Coleman on Unsplash